Haemorrhoids in Pregnancy: Understanding the Numbers and Risks
Pregnancy is a transformative journey, but for many expectant mothers, it is often accompanied by unexpected and uncomfortable physical changes. Among the most common yet rarely discussed issues is the development of haemorrhoids. Often referred to as “piles,” these swollen veins in the lower rectum and anus can cause significant distress during what should be a joyous time.
If you are currently experiencing discomfort, you are certainly not alone. At drchansh.my, we believe that understanding the scale and causes of this condition is the first step toward effective management and peace of mind. In this article, we delve into the epidemiology – the “numbers” – behind haemorrhoids in pregnancy and the specific risks that contribute to their prevalence.
The Scale of Haemorrhoids in Pregnancy: Epidemiology and Statistics
How common are haemorrhoids during pregnancy? According to the Proctology Depository, the prevalence of haemorrhoidal disease is remarkably high among the obstetric population.
A Wordwide Perspective
Global data suggests that while haemorrhoidal disease affects roughly 4% of the general population, these numbers skyrocket during pregnancy. Research indicates that up to 27.9% to 38.9% of pregnant women will experience symptomatic haemorrhoids at some point during their journey.
Some clinical reviews suggest that the figure may be even higher, with more than 50% of women developing symptoms either during the third trimester or in the immediate postpartum period (the weeks following childbirth).
A Timing of Symptoms
The prevalence of haemorrhoids is not uniform throughout the forty weeks of gestation. Epidemiological studies show a clear “crescendo” effect:
-
First Trimester: Symptoms are relatively rare, often related to pre-existing conditions or early-onset hormonal shifts.
-
Second Trimester: Prevalence begins to climb as the uterus expands.
-
Third Trimester: This is the “peak” period. The sheer physical weight of the foetus, combined with peak progesterone levels, makes this the most common time for symptomatic piles.
-
Postpartum: The “second peak” occurs immediately after delivery, often triggered by the intense physical strain of the second stage of labour (pushing).
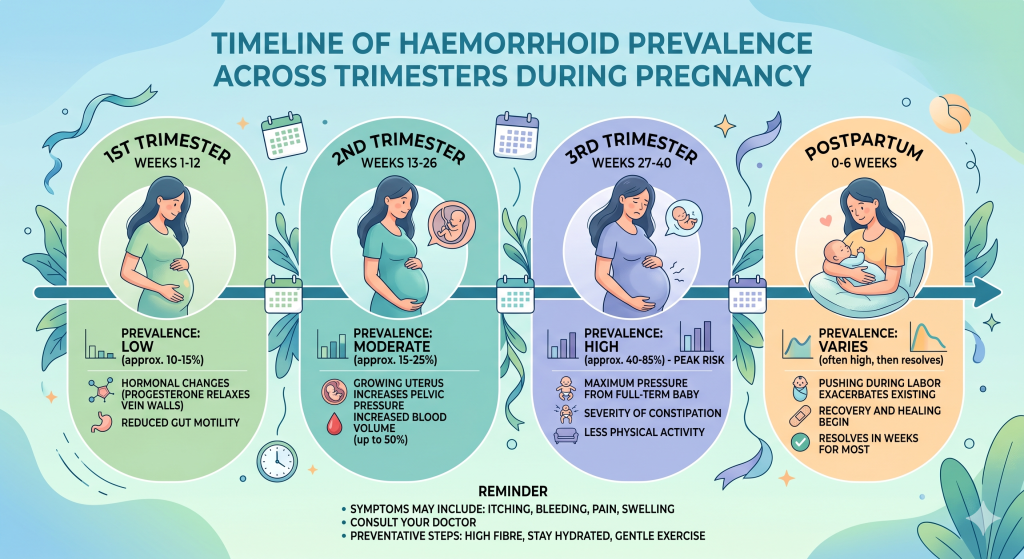
Figure 1: The rising prevalence of haemorrhoid symptoms as pregnancy progresses toward the third trimester and delivery.
Why Pregnancy? Identifying the Risk Factors
To understand why the numbers are so high, we must look at the physiological and mechanical changes that occur during pregnancy. Several factors converge to create the “perfect storm” for haemorrhoidal development.
1. Increased Blood Volume and Vascular Pressure
During pregnancy, a woman’s blood volume increases by approximately 40-50% to support the growing foetus. This extra volume increases the pressure within all blood vessels. Specifically, the growing uterus exerts direct pressure on the inferior vena cava, the large vein that returns blood from the lower body to the heart. This pressure causes “backflow” or pooling in the pelvic veins, leading to the swelling of the haemorrhoidal cushions.
2. Hormonal Changes (The Progesterone Factor)
The hormone progesterone is vital for maintaining a healthy pregnancy because it relaxes the smooth muscles of the uterus. However, it doesn’t just act on the uterus; it also relaxes the walls of the veins. When vein walls become more relaxed and “stretchy,” they are more prone to swelling and becoming engorged with blood, leading to haemorrhoids.
3. The Impact of Chronic Constipation
Epidemiological data shows a strong correlation between constipation and haemorrhoids in pregnant women. Progesterone slows down the digestive tract (motility), leading to harder stools. Additionally, the consumption of iron supplements—common in prenatal care—can further exacerbate constipation. The resulting straining during bowel movements is a primary mechanical cause of haemorrhoidal prolapse and bleeding.
4. The Strain of Labour
The “Numbers and Risks” of haemorrhoids would be incomplete without mentioning the act of childbirth itself. The intense intra-abdominal pressure during the pushing phase of labour can cause immediate swelling or thrombosis (clotting) of external haemorrhoids. Studies have shown that women who undergo a prolonged second stage of labour are at a significantly higher risk of developing postpartum haemorrhoids.
Classifying the Severity: The Goligher System
Medical professionals use the Goligher Grading System to categorise the severity of internal haemorrhoids. Understanding where you fall on this scale can help determine the necessary treatment:
-
Grade I: Internal haemorrhoids that bleed but do not prolapse (stay inside).
-
Grade II: Haemorrhoids that prolapse during bowel movements but retract spontaneously.
-
Grade III: Haemorrhoids that prolapse and require manual reduction (pushing them back in).
-
Grade IV: Haemorrhoids that are permanently prolapsed and cannot be reduced.
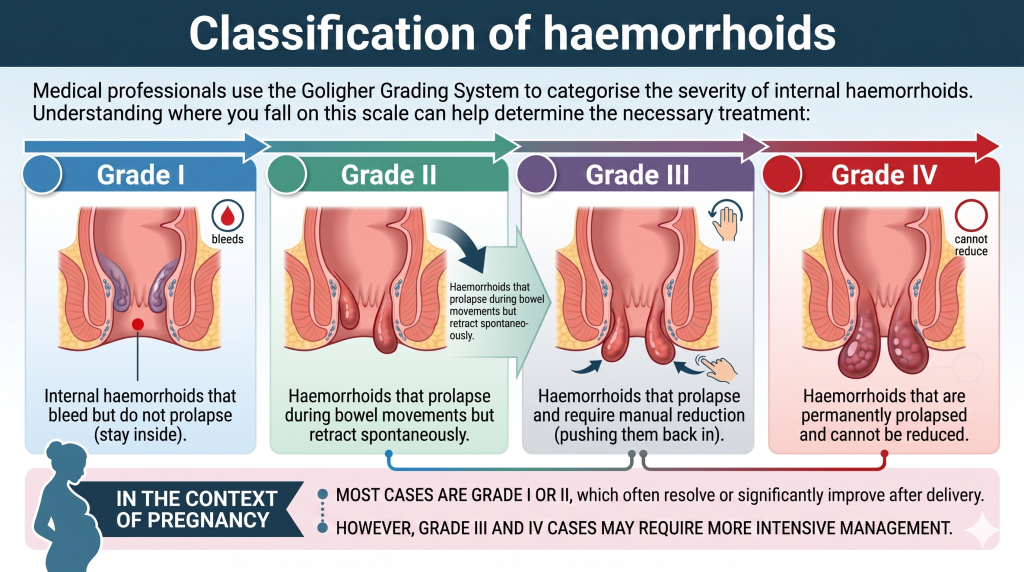
Figure 2: The four grades of haemorrhoidal disease, ranging from internal congestion to permanent prolapse.
In the context of pregnancy, most cases are Grade I or II, which often resolve or significantly improve after delivery. However, Grade III and IV cases may require more intensive management.
Long-term Risks and Quality of Life
While haemorrhoids are rarely life-threatening, their impact on Quality of Life (QoL) is substantial. Epidemiological studies using tools like the HEMO-FISS-CdV (Quality of Life questionnaire) reveal that pregnant women with haemorrhoids report:
-
Significant physical pain and itching (Pruritus Ani).
-
Disturbed sleep patterns.
-
Anxiety regarding bowel movements.
-
Decreased mobility.
It is important to note that left untreated, Grade III or IV haemorrhoids can lead to complications such as anaemia (due to chronic bleeding) or strangulation, where the blood supply to the haemorrhoid is cut off, causing intense pain.
Management and When to Seek Help
The good news is that for many women, pregnancy-related haemorrhoids are temporary. Management typically follows a “Treatment Ladder”:
-
Conservative Management: Increasing fibre intake, staying hydrated, and using stool softeners to reduce straining.
-
Pelvic Floor Physiotherapy: Using “pre-hab” exercises to strengthen the pelvic floor and improve circulation.
-
Topical Treatments: Emollient creams or ointments to soothe itching and inflammation.
-
Advanced Minimally Invasive Procedures: For those whose symptoms persist after pregnancy, modern techniques like Laser Haemorrhoidoplasty (LHP) offer a way to treat the condition with minimal pain and rapid recovery.
Conclusion: You Don't Have to Suffer in Silence

If you are struggling with symptoms, remember that relief is available. Monitoring your symptoms and seeking professional advice early can prevent the progression of the disease and ensure a more comfortable pregnancy and postpartum recovery. Don’t let discomfort hold you back. Schedule a consultation at drchansh.my today.
Figure 3: Pregnancy-related discomfort is common, but medical guidance can help manage the symptoms effectively.